



 Oligo Pools
Oligo Pools
 Variant Libraries
Variant Libraries





Get the latest by subscribing to our blog
There is, unfortunately, a difference between having no detectable cancer and being truly cancer free. Clinicians aim for the latter, but can usually only measure the former. This is largely due to our limited ability to detect cancer after treatment, when it’s in its most diminished state.
Molecular residual disease (MRD) testing has the potential to change this, offering a more sensitive alarm system for detecting persistent and recurring cancers. But if we’re going to realize this potential, the field will need more than a theoretically functional alarm system—we’ll also need the ability to effectively use it.
MRD Works; But Can It Actually Be Implemented?
We participated in a roundtable convened by The Scientist wherein experts came together to discuss the state of MRD and what it will take to turn the technology’s potential into clinical reality (you can watch the full webinar here). At the outset, the group agreed that the scientific foundation of MRD is strong, with ample evidence pointing to its potential to improve cancer detection and surveillance.
Often when tumors are first diagnosed, they’re large enough to be identified with radiological imaging (such as PET or CT scans). If treatment goes well, the tumor will shrink or altogether dissolve, its footprint in the body receding beyond the boundaries of what can be seen with imaging technology. Yet, that doesn’t mean the cancer is gone. For all the power they give us, the tools we use to detect and track cancer have limits; PET scans, for example, can’t detect individual tumor cells. This creates a biological penumbra, an uncertain space where tumors appear to be gone but where residual cancer cells may still grow beneath our notice. It's in this space that recurrent tumors gain a foothold.
MRD promises to do what imaging technology cannot. In the webinar, Dr. Ash Alizadeh from Stanford University explained “we have patients being treated with CAR-T cell therapy for large cell lymphomas, and their lymphoma is all gone. But they have exploding clonal hematopoiesis [a pre-malignant condition] that becomes secondary myeloid malignancies. We wouldn't have known about those if we weren't using [MRD assays] to monitor them.”
Designed to identify errant DNA released from individual tumor cells, MRD tests have the theoretical ability to detect recurrent tumors at their most nascent stages [1]. Doing so enables earlier and more informed therapeutic decision making [2,3]. Though no test has yet demonstrated the ability to track circulating tumor DNA back to a solitary malignant cell, many have proven to be extremely sensitive and have moved beyond the proof-of-concept stage for colorectal, lung, breast, urothelial and other cancer types [2,4-8].
“We wouldn't have known about those [cancers] if we weren't using [MRD assays].”– Dr. Ash Alizadeh
In the discussion, participants agreed that MRD is scientifically ready for prime-time, but they also emphasized what many in the field are coming to recognize: Several logistical barriers remain, which make broadscale implementation difficult. “The science is advancing very quickly,” explained BloodPac’s Executive Director Lauren Leiman, “but standards, workflows and the evidence frameworks needed for broad clinical and regulatory confidence are still catching up."
The Compromise No One Wants: Speed or Sensitivity?

One such barrier is the amount of time it takes to perform sensitive MRD workflows.
MRD assays use target capture probes—short segments of synthetic DNA that are designed to bind complementary portions of the tumor genome. When mixed with a pool of cell free DNA (sourced from a liquid biopsy sample), probes help to separate the rare tumor-derived DNA fragments from the far more numerous DNA fragments released from healthy cells. In doing so, capture probes enrich sequencing libraries for tumor DNA and have the potential to greatly improve the efficiency and sensitivity of the assay.
The most readily available MRD assays are off-the-shelf designs, where probes target sequences that are commonly present in a given cancer type (so called tumor-agnostic designs). With the economy of scale, these panels can be low in cost and ready-at-hand when needed. However, they also come with a significant tradeoff: Off-the-shelf panels can have reduced sensitivity and specificity because they may miss unique tumor mutations or produce false positives from non-malignant DNA.
In contrast, tumor-informed MRD panels use customized capture probes that are designed to target the unique mutations within individual tumor genomes. Not only does this increase the number of recognizable tumor-derived DNA fragments, but it also decreases the odds of false-positive hits, both of which greatly increase the assay’s sensitivity and specificity [9-12]. But, such a personalized design can take time to produce, time that patients may not have.
This tradeoff was highlighted in the webinar when Dr. Alizadeh described an experience he recently had with a patient in need of sensitive MRD testing during CAR-T treatment:
“This patient was walking on eggshells with me over this because we wanted to move to [a new panel design], but we would lose [critical] time if we did that.” If you can’t know whether a tumor has really gone, it’s hard to weigh the costs—both financial and physical—of continued treatment. Is additional therapy truly needed, or would it do more harm than good? Particularly when dealing with aggressive tumor types, these questions can loom over physicians like Alizadeh. “You need [MRD results] to come back quickly, on the order of days, not weeks.”
Operations Force A “Good Enough” Compromise
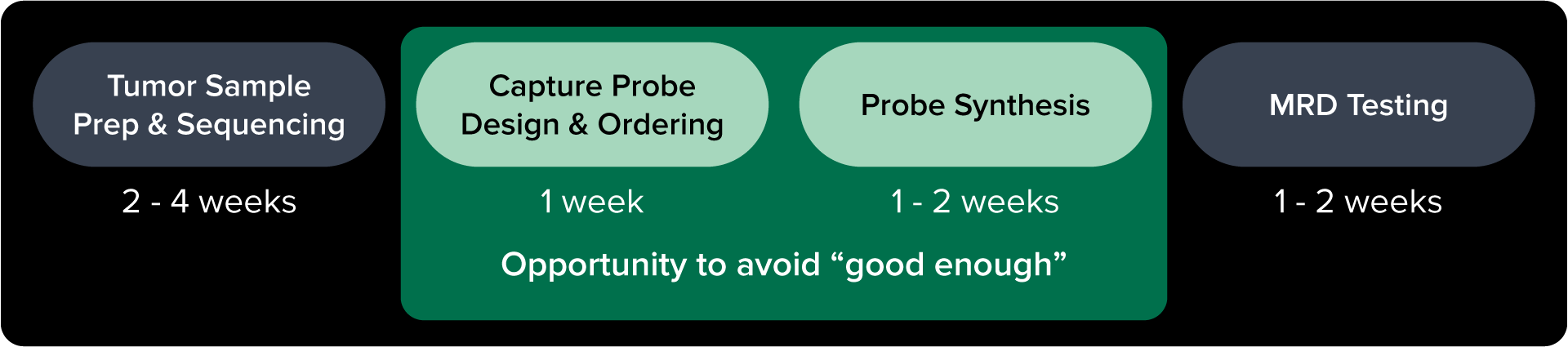
Many in the field believe that the need for speed in MRD testing is incompatible with customization. This is largely because customization has, historically, required considerably more work and time to accomplish. In the case of tumor-informed MRD panels, bespoke workflows have to be designed to perform sequencing of the patient's tumor; custom target probes have to be carefully designed according to the tumor sequencing results; probes must then be ordered, synthesized, and delivered.
Here the problem is not whether a personalized test can work, it’s whether it's feasible to use it. Fortunately, steps are already being taken to reduce the time and operational pains of this process.
For example, Twist has tools available specifically for designing probe sequences targeted to patient-specific markers. With its APIs and automated systems, Twist’s tools will take genomic context and translate it into the exact probe sequences that researchers may want to use in their tests.
Such tools can help make probe design far easier and quicker, enabling the high-throughput production that’s needed—a view reinforced in the webinar when Alizadeh shared what it's been like to use Twist’s probe design tools.
Twist is also working to improve the speed of bespoke panel synthesis. As stated by Alizadeh, waiting for custom enrichment probes to be synthesized and delivered can sometimes take weeks. Particularly when facing an aggressive cancer, the time needed for customization makes it impractical for most. That’s why researchers at Twist are working to enable a 24 hour turnaround from the time that researchers submit their probe design to the time the probes are shipped out. It is hoped that this quick turnaround time may help provide the speed of tumor-agnostic assays with the ultrasensitivity of tumor-informed assays.
Collectively, these innovations can help remove major barriers that currently limit adoption of tumor-informed MRD testing.
🔎 Operational Improvements Needed
In the roughly 1 hour discussion, experts touched on many operational challenges that need to be addressed for MRD to be successfully adopted on a broader scale (in addition to the customization barrier discussed here). These challenges included standardization of lexicon, quality metrics, benchmarking studies, and bespoke bioinformatics pipelines. For high-throughput applications, MRD panel providers will also need to ensure they’re delivered in automation-friendly formats.
Learn about these challenges—along with some potential solutions—by tuning in to the discussion here >>
Prepare For MRD By Optimizing Operations
The collective evidence suggests that MRD is ready for primetime. There are of course situations where MRD has yet to prove itself, but these are increasingly viewed as the exception rather than the rule [8,13]. It is therefore important for labs to shift from simply validating that MRD assays can work, to building the robust infrastructure and workflows that are needed to actually use such a valuable tool.
In the webinar, experts described several steps that will need to be taken by the field to realize the potential of MRD. Improving the manufacturing of target capture probes was one such step. If we can deliver customized capture panels with minimal friction and rapid turnaround, researchers may no longer need to choose between sensitivity and speed.
Watch the panel discussion to learn more about the future of MRD and how Twist is helping to address the field’s looming operational challenges.
References
1.Northcott, Josette, et al. “Analytical Validation of next Personal ® , an Ultra-Sensitive Personalized Circulating Tumor DNA Assay.” Oncotarget, vol. 15, 6 Jan. 2024, pp. 200–218, https://doi.org/10.18632/oncotarget.28565.
2.Boukouris, Aristeidis E., et al. “A Comprehensive Overview of Minimal Residual Disease in the Management of Early-Stage and Locally Advanced Non-Small Cell Lung Cancer.” Npj Precision Oncology, vol. 9, no. 1, 13 June 2025, https://doi.org/10.1038/s41698-025-00984-9.
3.Song, Meiling, et al. “Minimal Residual Disease Detection: Implications for Clinical Diagnosis and Cancer Patient Treatment.” MedComm, vol. 6, no. 6, 15 May 2025, https://doi.org/10.1002/mco2.70193.
4.Puddu, Fabio, et al. “5-Methylcytosine and 5-Hydroxymethylcytosine Are Synergistic Biomarkers for Early Detection of Colorectal Cancer.” Communications Medicine, vol. 6, no. 1, 20 Jan. 2026, https://doi.org/10.1038/s43856-025-01278-8.
5.Black, James R. M., et al. “Ultrasensitive CtDNA Detection for Preoperative Disease Stratification in Early-Stage Lung Adenocarcinoma.” Nature Medicine, 13 Jan. 2025, https://doi.org/10.1038/s41591-024-03216-y.
6.Berry, Donald A., et al. “Association of Minimal Residual Disease with Clinical Outcome in Pediatric and Adult Acute Lymphoblastic Leukemia.” JAMA Oncology, vol. 3, no. 7, 13 July 2017, p. e170580, https://doi.org/10.1001/jamaoncol.2017.0580.
7.Mehler, Shoshana, et al. “Performance Characteristics of a Tumor-Informed Circulating Tumor DNA (CtDNA) Minimal Residual Disease (MRD) Assay in Invasive Bladder Cancer in Clinical Practice.” Journal of Clinical Oncology, vol. 41, no. 6_suppl, 20 Feb. 2023, pp. 542–542, https://doi.org/10.1200/jco.2023.41.6_suppl.542.
8.Abdo, Theresa, et al. “Minimal Residual Disease in Solid Tumors: Clinical Applications and Future Directions.” Cancer, vol. 132, no. 3, 28 Jan. 2026, https://doi.org/10.1002/cncr.70286.
9.Martínez-Castedo, B., et al. “Minimal Residual Disease in Colorectal Cancer. Tumor-Informed versus Tumor-Agnostic Approaches: Unraveling the Optimal Strategy.” Annals of Oncology, 13 Dec. 2024, https://doi.org/10.1016/j.annonc.2024.12.006.
10.Dong, Qiantong, et al. “Clinical Application of Molecular Residual Disease Detection by Circulation Tumor DNA in Solid Cancers and a Comparison of Technologies: Review Article.” Cancer Biology & Therapy, vol. 24, no. 1, 13 Nov. 2023, https://doi.org/10.1080/15384047.2023.2274123.
11.Nguyen Hoang, Van-Anh, et al. “Direct Comparison of Tumor-Informed and Tumor-Naive Circulating Tumor DNA Assays for Recurrence Detection in Early-Stage NSCLC.” JTO Clinical and Research Reports, vol. 7, no. 1, Jan. 2026, p. 100927, https://doi.org/10.1016/j.jtocrr.2025.100927.
12.Santonja, Angela, et al. “Comparison of Tumor‐Informed and Tumor‐Naïve Sequencing Assays for CtDNA Detection in Breast Cancer.” Embo Molecular Medicine, vol. 15, no. 6, 10 May 2023, https://doi.org/10.15252/emmm.202216505.
13.Hu, Qiugen, et al. “Circulating Tumor DNA: Current Implementation Issues and Future Challenges for Clinical Utility.” Clinical Chemistry and Laboratory Medicine, vol. 0, no. 0, 19 Dec. 2023, https://doi.org/10.1515/cclm-2023-1157

Twist Bioscience HQ
681 Gateway Blvd
South San Francisco, CA 94080